IADR Abstract Archives
Is Craniofacial Anatomy Related to the Severity of Paediatric OSA?
Objectives: To investigate the relationship between either the severity of obstructive sleep apnoea (OSA), or the degree of upper airway obstruction, and a series of dentoskeletal, soft tissues, and airway parameters in children and adolescents of Hong Kong.
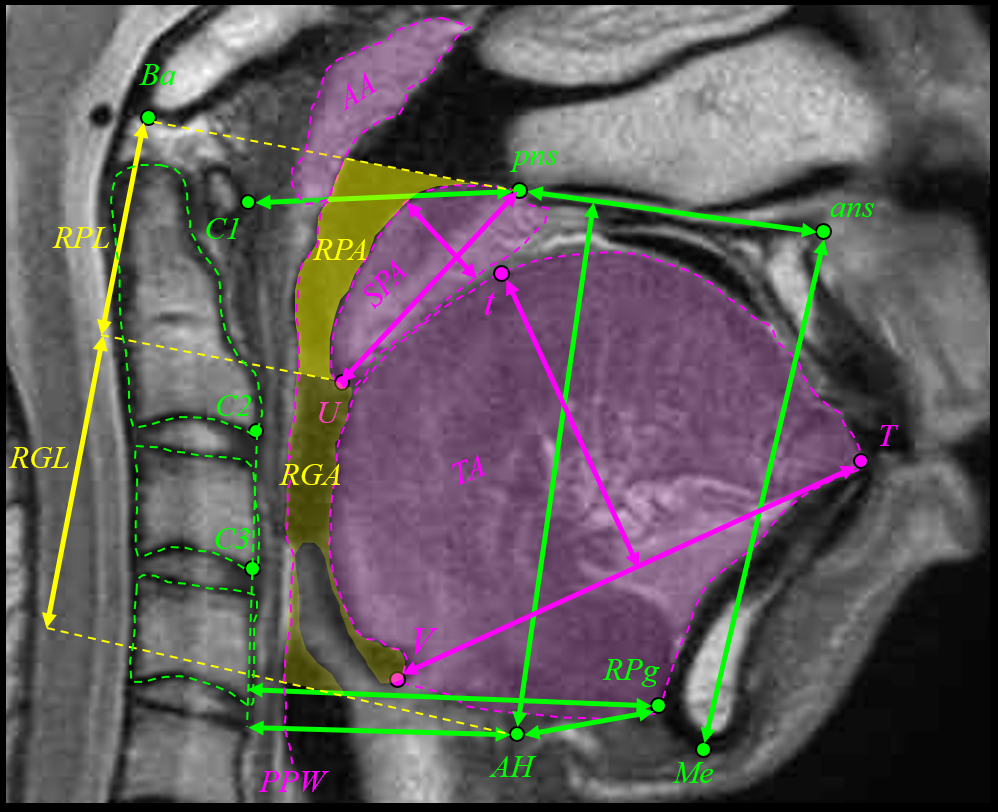
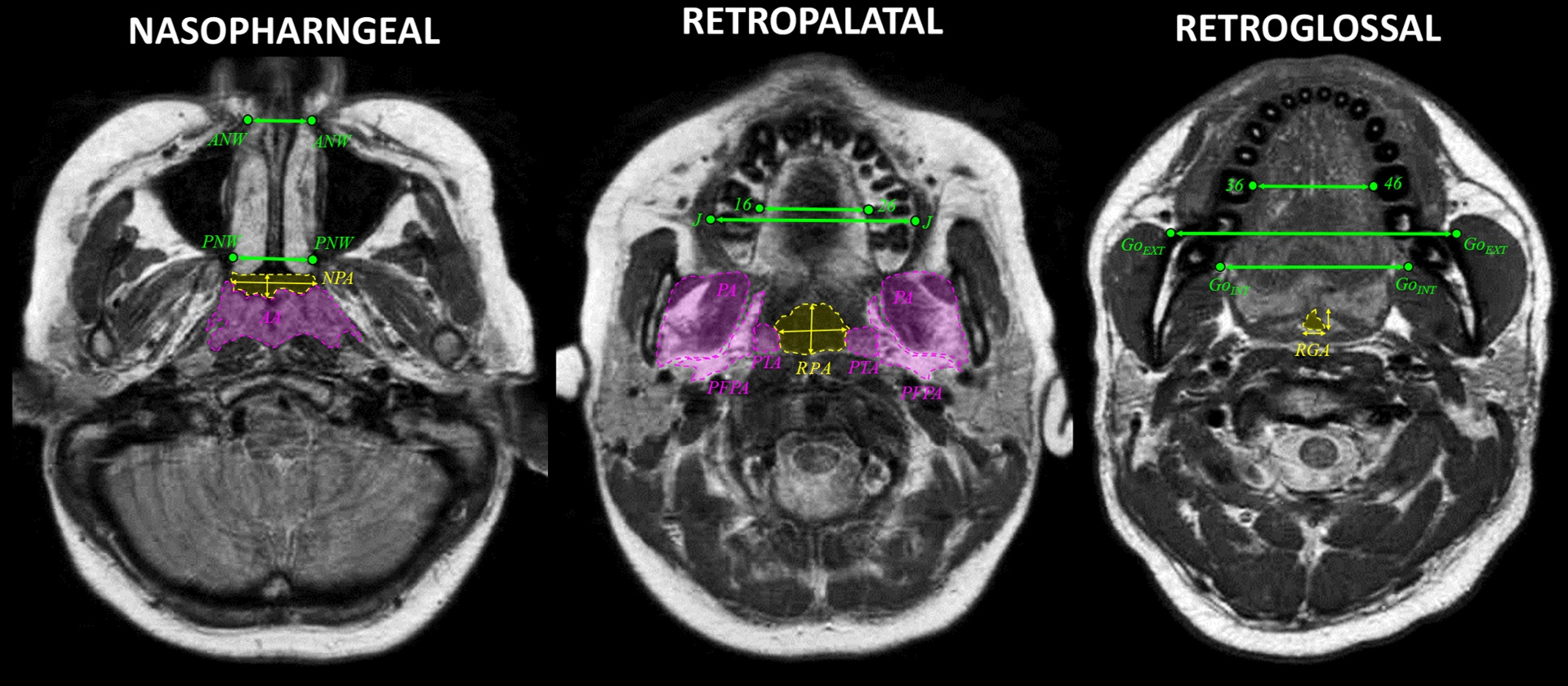
Methods: Twenty-five patients (22 males, 3 females, mean age 13.4±3.1 years, 8 to 18-year-old,), with OSA were retrospectively analysed. OSA was diagnosed with polysomnography as apnoea-hypopnoea index (AHI) >1 event/hour (mean AHI 4.3±5.9 events/hour, 1.0 to 30.1 events/hour). Kinetic magnetic resonance imaging (kMRI) during drug-induced sleep was used to assess the dynamic airway patency and the obstruction type. Static MRI (sMRI) was also used for measuring dentoskeletal, soft tissue, and airway parameters. Factors related to OSA and obstruction severity were identified with multiple linear regression adjusted for age, sex, height, skeletal maturation, and body-mass index or axial parapharyngeal-fat-pads area (significance α=0.05).
Results: From kMRI, circumferential obstruction was present in 44% of patients, while latero-lateral and antero-posterior in 28%. From kMRI, obstructions were retropalatal in 64% of cases and retroglossal in 36% (no nasopharyngeal obstruction was present). A difference was present between kMRI and sMRI in assessing the obstruction level (p=0.037), with kMRI showing higher prevalence of retroglossal obstructions. The airway area of the main obstruction site was not related to AHI. The maxillary basal latero-lateral width was related to both AHI (β=-0.573, p=0.008) and dynamic obstruction during sleep (β=0.633, p=0.011). Similarly, the maximum retropalatal latero-lateral width was related to both AHI (β=-0.408, p=0.040) and dynamic obstruction during sleep (β=0.515, p=0.016).
Conclusions: In children and adolescents, the severity of OSA and the amount of dynamic obstruction were inversely proportional to the basal width of the maxilla and to the static retropalatal width of the airway. Targeted clinical treatments widening the transverse dimension of these structures may be particularly beneficial to these patients.
Methods: Twenty-five patients (22 males, 3 females, mean age 13.4±3.1 years, 8 to 18-year-old,), with OSA were retrospectively analysed. OSA was diagnosed with polysomnography as apnoea-hypopnoea index (AHI) >1 event/hour (mean AHI 4.3±5.9 events/hour, 1.0 to 30.1 events/hour). Kinetic magnetic resonance imaging (kMRI) during drug-induced sleep was used to assess the dynamic airway patency and the obstruction type. Static MRI (sMRI) was also used for measuring dentoskeletal, soft tissue, and airway parameters. Factors related to OSA and obstruction severity were identified with multiple linear regression adjusted for age, sex, height, skeletal maturation, and body-mass index or axial parapharyngeal-fat-pads area (significance α=0.05).
Results: From kMRI, circumferential obstruction was present in 44% of patients, while latero-lateral and antero-posterior in 28%. From kMRI, obstructions were retropalatal in 64% of cases and retroglossal in 36% (no nasopharyngeal obstruction was present). A difference was present between kMRI and sMRI in assessing the obstruction level (p=0.037), with kMRI showing higher prevalence of retroglossal obstructions. The airway area of the main obstruction site was not related to AHI. The maxillary basal latero-lateral width was related to both AHI (β=-0.573, p=0.008) and dynamic obstruction during sleep (β=0.633, p=0.011). Similarly, the maximum retropalatal latero-lateral width was related to both AHI (β=-0.408, p=0.040) and dynamic obstruction during sleep (β=0.515, p=0.016).
Conclusions: In children and adolescents, the severity of OSA and the amount of dynamic obstruction were inversely proportional to the basal width of the maxilla and to the static retropalatal width of the airway. Targeted clinical treatments widening the transverse dimension of these structures may be particularly beneficial to these patients.
IMAGES
3648342_File000000.jpg
3648342_File000001.jpg
3648342_File000000.jpg
3648342_File000001.jpg