IADR Abstract Archives
An Analysis of Aerosol Emissions From Dental Procedures.
Objectives: In this study, we aimed to quantify total aerosol concentration (TAC) produced during different dental procedures. Where aerosol was detected, we assessed whether the aerosol size distribution from patient procedures was explained by the non-salivary contaminated instrument source, using phantom head controls.
Methods: This study obtained ethical approval as part of the AERATOR grant. Patients were recruited consecutively via telephone and written consent was obtained. Both an optical and an aerodynamic particle sizer were used to measure aerosol, attached to a 3D-printed polylactide funnel 22cm from the patients face. A range of periodontal, oral surgery and orthodontic treatments were captured using sample time-stamped protocols. High-fidelity phantom head control experiments for each procedure were also performed, under the same conditions.
TAC was measured for each procedure. For those which registered above background, phantom control and patient procedure aerosol size distributions were compared, with the assumption that if the distributions were the same, all aerosol detected from the patient could be explained by the instrument source. To further assess if size distributions differed other than by chance, a two-sided unpaired t-test was used, with a Bonferroni corrected p-value of <0.002 considered significant.
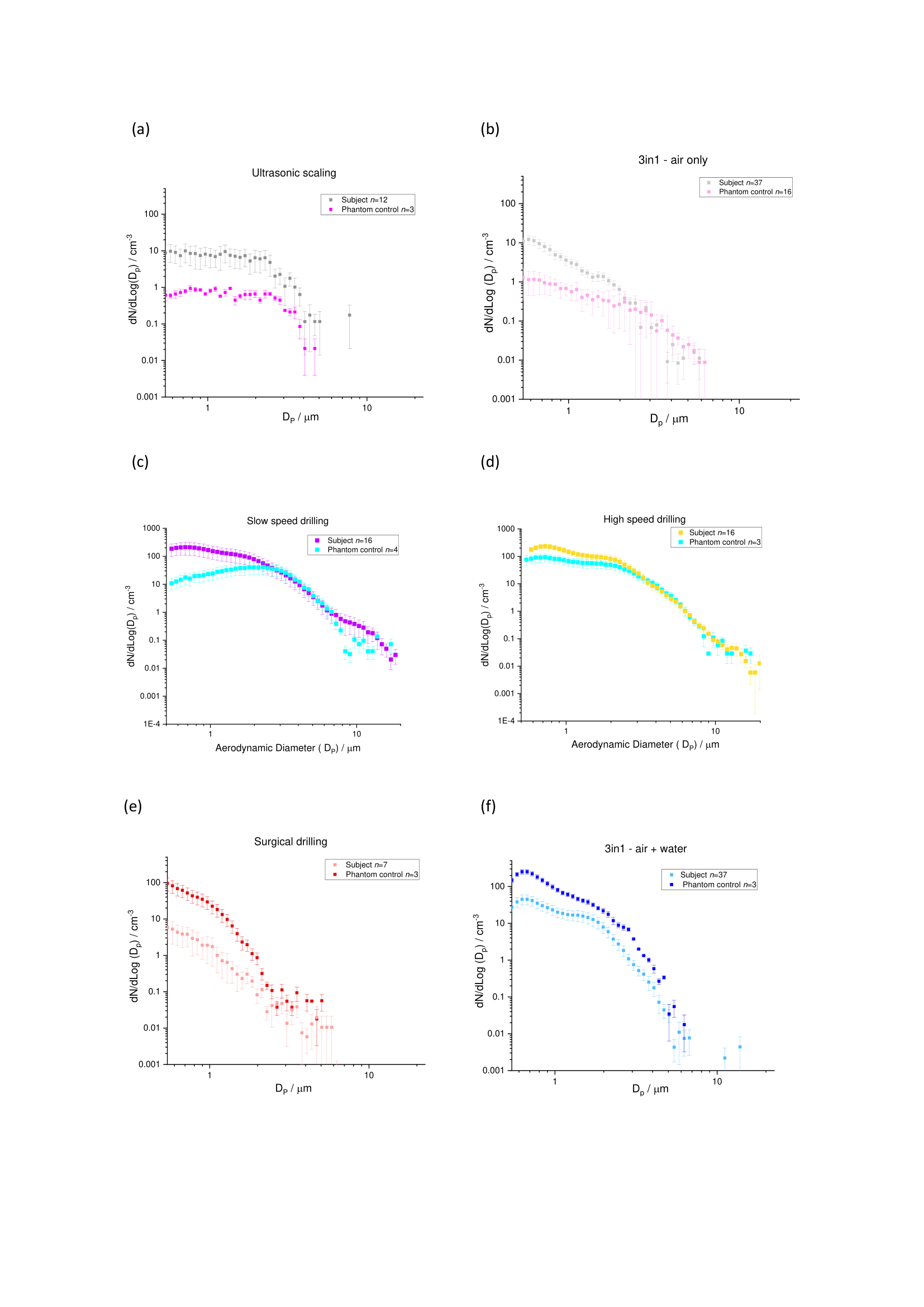
Results: 41 patients underwent 12 different dental procedures. Aerosol was detect for 5 procedures and for these the percentage of procedure time that aerosol was observed above background ranged from 12.7% for ultrasonic scaling to 42.9% for 3in1 air+water (Table 1). High-speed drilling produced 10-fold greater TAC compared to the other procedures. No differences were detected between phantom control and patient procedure size distributions for ultrasonic scaling, 3in1 air/air+water, or surgical drilling. However, there was a statistically significant difference in size distributions for high (p=1.10x10-5) and slow-speed drilling (p=5.54x10-8), with additional unexplained aerosol also present (Figure 1).
Conclusions: It is evident that several common dental procedures generate aerosol, but for most this can be explained by the non-salivary contaminated instrument source. However, aerosol from slow speed drilling could not be fully explained and so risk here cannot be excluded.
Methods: This study obtained ethical approval as part of the AERATOR grant. Patients were recruited consecutively via telephone and written consent was obtained. Both an optical and an aerodynamic particle sizer were used to measure aerosol, attached to a 3D-printed polylactide funnel 22cm from the patients face. A range of periodontal, oral surgery and orthodontic treatments were captured using sample time-stamped protocols. High-fidelity phantom head control experiments for each procedure were also performed, under the same conditions.
TAC was measured for each procedure. For those which registered above background, phantom control and patient procedure aerosol size distributions were compared, with the assumption that if the distributions were the same, all aerosol detected from the patient could be explained by the instrument source. To further assess if size distributions differed other than by chance, a two-sided unpaired t-test was used, with a Bonferroni corrected p-value of <0.002 considered significant.
Results: 41 patients underwent 12 different dental procedures. Aerosol was detect for 5 procedures and for these the percentage of procedure time that aerosol was observed above background ranged from 12.7% for ultrasonic scaling to 42.9% for 3in1 air+water (Table 1). High-speed drilling produced 10-fold greater TAC compared to the other procedures. No differences were detected between phantom control and patient procedure size distributions for ultrasonic scaling, 3in1 air/air+water, or surgical drilling. However, there was a statistically significant difference in size distributions for high (p=1.10x10-5) and slow-speed drilling (p=5.54x10-8), with additional unexplained aerosol also present (Figure 1).
Conclusions: It is evident that several common dental procedures generate aerosol, but for most this can be explained by the non-salivary contaminated instrument source. However, aerosol from slow speed drilling could not be fully explained and so risk here cannot be excluded.
IMAGES
3602000_File000001.jpg
3602000_File000001.jpg