IADR Abstract Archives
Prosthetic Treatment Modalities in Patients With Head and Neck Radiotherapy
Objectives: Radiotherapy (RT) for head and neck (H&N) cancer can pose multiple challenges. We must minimize risk of osteoradionecrosis (ORN) from oral surgeries, tissue trauma, and complications from xerostomia, trismus, neuromuscular disorder or anatomical changes, but maximize the reconstruction goal. Prosthesis are crucial for reconstructing post-radiation dental lesions and long-span edentulism. This case series evaluated H&N RT patients who underwent successful oral surgeries and full mouth rehabilitation, with altered vertical dimension (VD).
Methods: Five H&N cancer patients who received RT were included. Two years after RT completed, oral rehabilitation was planned due to compromised masticatory function. Proper wound management was done for oral surgeries to prevent ORN. The distribution of edentulous area, jaw relationship, abutment selections were analyzed for prosthesis fabrication.
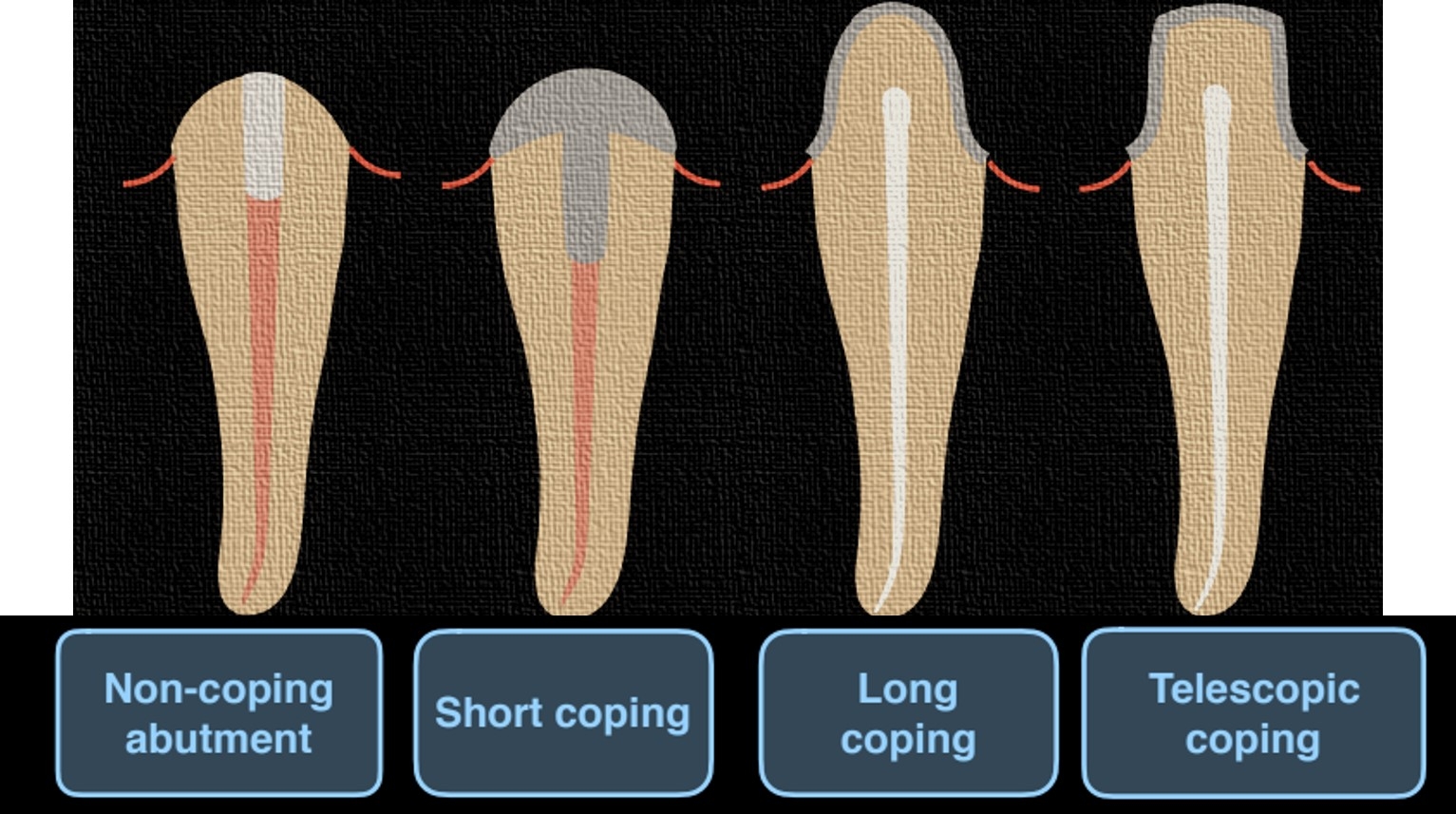
Patients 1~4 received removable partial dentures (RPDs) with combination of either casted or resin root copings and surveyed fixed partial dentures (FPDs). Patient 5 received full mouth FPDs to halt dentition breakdown.
Results: Patients who underwent H&N RT may have higher caries rate, xerostomia, and more susceptible to other complications leading to compromised dentition. Risk of ORN was also a concern for oral surgeries, but can be reduced by choices of surgical region, number of extracted teeth, and application of root copings. Evaluation of soft/hard tissue, abutment prognosis are essential, so key abutments can be selected to enhance function of RPDs. Altering VD can benefit in esthetic concern, relieve angular cheilitis, and improve post-RT dental lesions resulted from impaired structures and components of the teeth and decreased salivation.
Conclusions: Our case series demonstrated that proper management of surgical wound, well-designed prosthesis can provide successful oral rehabilitation. Through patients’ tremendous hygiene care, the residual dentitions and mucosal surfaces remain intact, without further RT-related complication occurred for the following period.
Methods: Five H&N cancer patients who received RT were included. Two years after RT completed, oral rehabilitation was planned due to compromised masticatory function. Proper wound management was done for oral surgeries to prevent ORN. The distribution of edentulous area, jaw relationship, abutment selections were analyzed for prosthesis fabrication.
Patients 1~4 received removable partial dentures (RPDs) with combination of either casted or resin root copings and surveyed fixed partial dentures (FPDs). Patient 5 received full mouth FPDs to halt dentition breakdown.
Results: Patients who underwent H&N RT may have higher caries rate, xerostomia, and more susceptible to other complications leading to compromised dentition. Risk of ORN was also a concern for oral surgeries, but can be reduced by choices of surgical region, number of extracted teeth, and application of root copings. Evaluation of soft/hard tissue, abutment prognosis are essential, so key abutments can be selected to enhance function of RPDs. Altering VD can benefit in esthetic concern, relieve angular cheilitis, and improve post-RT dental lesions resulted from impaired structures and components of the teeth and decreased salivation.
Conclusions: Our case series demonstrated that proper management of surgical wound, well-designed prosthesis can provide successful oral rehabilitation. Through patients’ tremendous hygiene care, the residual dentitions and mucosal surfaces remain intact, without further RT-related complication occurred for the following period.
IMAGES
4000325_File000000.jpg
4000325_File000000.jpg